
In the late 50s, Sir James Black Cardiovascular therapy revolutionized With your new treatment: beta blockers. A medication that has been the immovable pillar in current medicine for patients with an acute myocardial infarction in their history. But now, A series of studies They have arrived to change the idea we had about the administration of this treatment.
A group of patients more affection. Studies published in the most prestigious medical magazines, such as The New EnglandThey arrive to draw a much more complex and personalized panorama of treatment administration. And he has reached such an extent that he suggests that for some people with a very specific clinical profile, and especially in women, their administration may not be necessary.
Why are the beta blockers. To understand the magnitude of this change, you have to travel in time. The studies that cemented the use of beta blockers were carried out in the 80s, a very different era for cardiology. At that time, a heart attack was much less aggressive.
There were no urgent angioplasties with stents to open obstructed arteries, nor the general use of High power statins either antiplatelet therapies dual In that context, the beta blockers demonstrated reduce mortality by an impressive 23%.
A question in the air. Today, the standard treatment of a heart attack is radically different and much more effective. The question that floated in the air for years was: in this new era, are they still the universally necessary beta blockers, especially for those patients whose heart has not been seriously damaged?
A concept that is key. To understand the great advance that has been made, you have to know what the left ventricular ejection fraction (FEVI). You can think like the “power percentage” that the heart has to expel the blood from the left ventricle to the aorta and by entity towards the coronary vessels of the heart. In this way, there are two scenarios right now on the table:
- Patient with a reduced fevi (≤40%): the heart has been weakened. In this group, no one doubts the benefit of the beta blockers since the evidence is solid.
- Patient with a non -reduced FEVI (> 40%): The heart maintains a good pumping force after infarction. It is here that the great debate has emerged around whether it is necessary to apply or not beta blockers so that they have a beneficial effect.
THE REBOOT TEST. The first great protagonist of this new story is the reboot essaya massive study conducted in Spain and Italy with more than 8,500 patients. All participants had suffered an acute myocardial infarction, but had a FEVI greater than 40%. Half of these received beta blockers and the other half not.
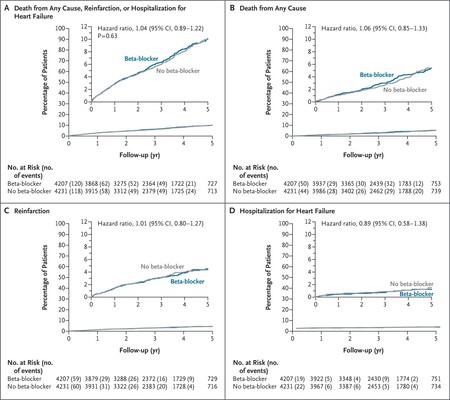
After a follow -up of 3.7 years, the results were overwhelming: there was no statistically significant difference between the two study groups. The Beta blocker group had an event rate of 22.5 per 1000 patients-year, compared to 21.7 in the group without them. Statistically, a technical draw.
Beta blocker effect on women. Reboot analysis by sexwhich included 1,627 women, revealed a significant interaction. In men, the beta blockers showed neither benefit or harm. The event rate was practically identical, with or without treatment.
In women, the result was radically different. Those who took beta blockers had a relative risk of 45% greater to suffer the main combined event with which they did not take them.
Concentrated in two groups. This excess risk in women was mainly driven by an increase in mortality due to any cause. The study also discovered that this potential damage was concentrated in two subgroups: women with FIVI preserved (≥50%) and women who received higher doses of beta blockers.
The researchers suggest that there could be pharmacokinetic reasons behind this. At equivalent doses, women tend to reach higher concentrations of the drug in blood due to physiological differences such as lower body weight and different metabolism. This could lead to adverse effects not seen in men with the same doses. Although it is something that will have to continue deepening.
Studies that are opposite. The grace of science is that opposite results can be found on the same topic. And just when the reboot result seemed to sentence the debate, the results of the twin trials were published Betami and Danblock made in Norway and Denmark with almost 5,600 participants. With a similar design (patients with IAM and FEVI ≥40%) their conclusions were different.
In this case, the treatment with beta blockers did demonstrate a benefit, reducing the risk of the primary objective (a death combined, major cardiovascular events, unplanned revascularization, stroke …). The incidence was 14.2% in the group with beta blockers compared to 16.3% in the control group.
When the data broken down, the main engine of this benefit was a significant reduction in the incidence of a new myocardial infarction: 5% vs. 6.7%. Interestingly, and in direct contrast with reboot’s findings, its subgroup analysis showed that the benefit seemed more pronounced in women.
A meta -analysis to find the midpoint. We have two mass studies, well designed and with opposite results. How do we solve this apparent contradiction? For this we use the most powerful tool of scientific evidence: a meta -analysis of individual patient data.
An international team, led by the researchers of the previous essays, decided to combine strength. They combined the data of reboot patients, Betami, Danblock and a fourth smallest study (capital-RCT) to focus on a very specific group: those with slightly reduced FEVI (between 40% and 49%). This is the “gray area”, patients who do not have seriously damaged heart, but not completely normal.
A surprising result. When analyzing the 1,885 patients who fit in this profile, the conclusion was clear: in this subgroup, the beta blockers are beneficial. A 25% reduction was seen in the risk of having a heart attack, heart failure or dying. In addition, the Hazard Ratio (a risk measure) was 0.75, indicating a clear and statistically significant protective effect.

Beta blockers continue to work. Despite the idea that can be infused that beta blockers are useless, the reality is that there are several points that can serve as a conclusion of these studies:
- If the FIVI is reduced (≤40%), the heart is weak and the beta blockers remain absolutely crucial. There are no doubt here.
- If FEVI is slightly reduced (40-49%): the heart is in an intermediate zone. The new meta -analysis demonstrates in a robust way that this group clearly benefits from the treatment with beta blockers.
- If the FIVI is preserved (≥50%): the heart pumps strongly. This is where the evidence suggests that beta blockers probably do not contribute any significant benefit. The reboot essay, the largest to date, found no advantage in this majority group
- If you are a woman with Fevi preserved: you have to be especially cautious. The reboot study has lit an alarm light on a possible increase in risk, which could lead doctors to reconsider dose or even the need for treatment in this patient profile
The cardiologists have reacted. Felipe Díez del Hoyo, an interventionist cardiologist, commented these Results in your X account highlighting the scientific level that is right now in Spain. Under his point of view, and seeing the results, he believes that with Fevi> 50% and a complete revascularization after the infarction the beta blockers do not provide benefit.
It does not mean that you have to leave the treatment. Logically, these studies mark a precedent to study to edit clinical guides in the pharmacological treatment after an IAM. But this does not mean that patients should suspend their treatments after seeing these publications, but always consulting medical professionals who will always guide the best treatment based on more solid scientific evidence.
Images | Ali Hajiluyi Towfiqui Barbhuiya
In Xataka | It is not the speed when remembering words, it is the speed at which we talk: the new track about dementia
GIPHY App Key not set. Please check settings